Flat Adenoma Resection Instrument (FARIn)
for
en-bloc resektion large lesions near Muskolaris propria
The „Flat Adenoma Resection Instrument (FARIn)“ was developed to treat especially large polyp-like and flat lesions > 2 cm bis ca. 4 cm en bloc near the muscularis propria and with low mechanical and thermal artifacts in a short time (pure resection time without marking, re-injection and cutting, < 1 min.) to be able to resect.
An important reason for the development of these instruments was and is the requirements of oncology. Resection of pathological tissue areas of the mucosa or submucosa of the gastrointestinal tract in sano, as well as the requirements of pathology en-bloc and without mechanical and thermal artifacts in the resectate.
A new procedure called Endoscopic Submucosa Resection (ESR) and new instruments (FARIn) are now available. the clinical applications after extensive in vitro testings was successful for CE-marking.
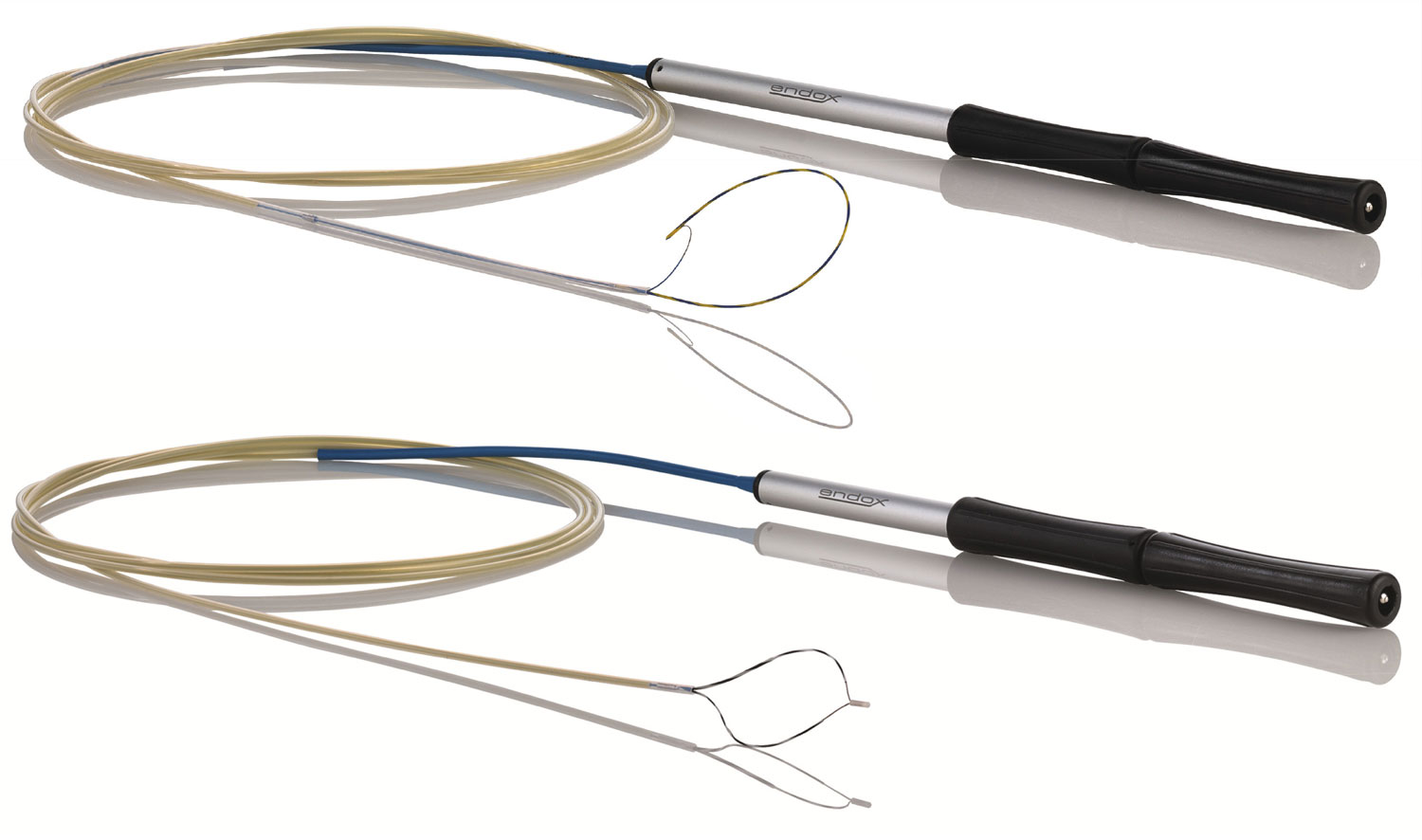
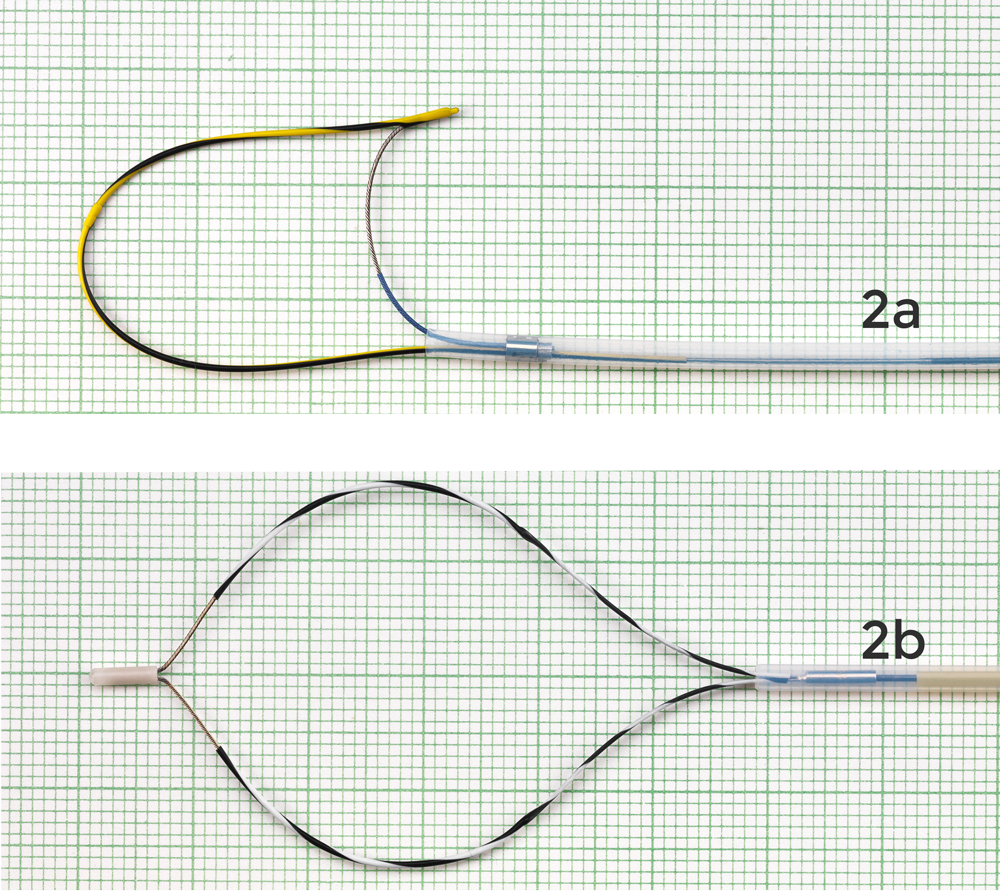
The most important feature of these instruments is the effector, which is available both as an asymmetrically opening and closing (Fig. 2a) and as a symmetrically opening and closing (Fig. 2b) HF surgical resection loop.
More details you can find out on the product sheet (PDF-Download)
At the specialized publishing house - © Georg Thieme Verlag KG Stuttgart · New York - is an article in the magazine "Endoscopy ( 2016; 48(S 01): E218-E219 )" appeared.
To the publication (external Link!)
... more info
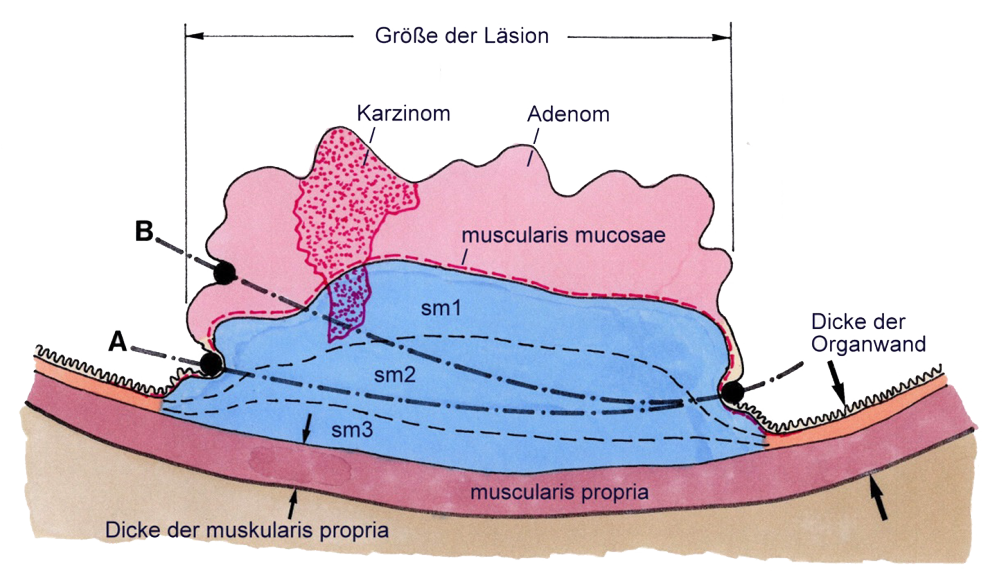
1. The effector or the sling must not be exposed to the organ wall is pressed. A cut in the direction of the organ wall or muscularis propria can be used with the asymmetrical sling thanks to the electrical insulation of and the spur, and with the symmetrical sling thanks to the electrical insulation of the loop sections and the electrically insulated skid not possible if used as intended. The cut can be made plane-parallel to the muscularis propria. After injection of the lesion and swelling of Submucosa can be found there, and of course only there, where the shape of the organ wall or Muscularis propria is suitable for this, e.g. stomach, rectum, caecum, the incision below the sm1. The symmetrical effector can also be used depending on the localization, size and morphology of the lesion can also be applied in the colon.
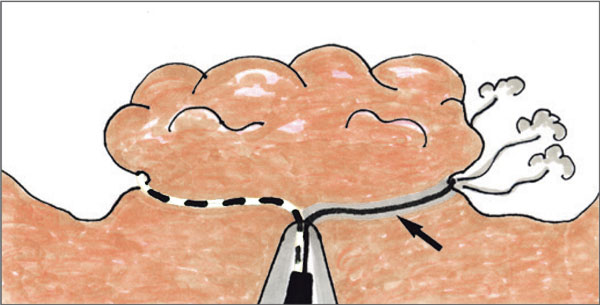
Usual incision with conventional polypectomy loops in direction away from the organ wall (B) and now possible incision with a FARIn (A)
2. Probably less thermal and/or mechanical artifacts in the resectate-side submucosa than in ESD
3. Thanks to the short cutting wire, only a low HF current is required, especially during the gating phase. There is no dangerous delay of the incision and consequently no thermal damage to the organ wall.
4. Since the length of the effective cutting wire of both the asymmetrical and symmetrical effectors remains constant at 1.5 cm during the entire cut, a constant cut quality can be achieved over the entire cut surface.
5. There is no uncontrolled cut due to spring elastic relaxation of the resection loop, which is unavoidable with conventional polypectomy loops.
6. For efficient cut-synchronous vessel occlusion, the relevant cutting speed of the vessel supply below the respective lesion may be adjusted. The slower the cutting speed, the more effective the vascular occlusion. With the FARIn, controlled cutting can be performed as fast or as slow as desired, depending on the vascular supply and the intended cut-synchronous vascular occlusion.
7. The reproducibility of the HF-surgical parameters (settings on HF-surgical units) is ensured thanks to the FARIn models, which are already available and will be available in the future, and thanks to a standardized and constant length of the cutting wire (1.5 cm) for all models.
8. The novel manipulation handle enables precise opening and closing as well as manipulation of the effector in axial and rotational direction.
The HF surgically active cutting wire of the ENDOx sling is approximately 50% shorter than that of comparably large but non-insulated slings. This makes the incision delay much shorter. Moreover, the risk of an incision in the direction of the organ wall is only half as high with the ENDOx sling as with conventional polypectomy slings. This makes the ENDOx sling particularly suitable for the removal of large polyps.
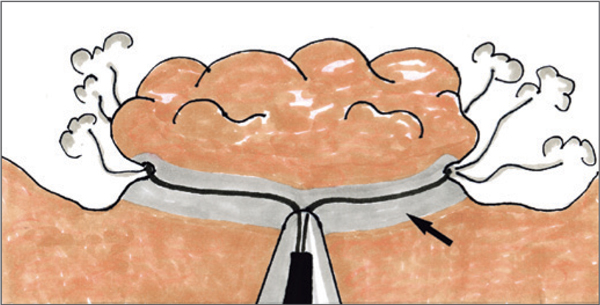 When using conventional polypectomy loops on large polyps (> 1cm), long incision delays can cause large and deep thermal tissue damage (coagulation plus devitalization zones) (see arrow).
When using conventional polypectomy loops on large polyps (> 1cm), long incision delays can cause large and deep thermal tissue damage (coagulation plus devitalization zones) (see arrow).
 When using ENDOx resection loops, the incision delay is relatively short even on large polyps (> 1 cm) and consequently the thermal tissue damage (coagulation plus adjacent devitalization zones) is relatively small and not deep (see arrow).
When using ENDOx resection loops, the incision delay is relatively short even on large polyps (> 1 cm) and consequently the thermal tissue damage (coagulation plus adjacent devitalization zones) is relatively small and not deep (see arrow).